
Dislocation of the Mandible / Jaw Dislocation / TMJ Subluxation
Dislocation of the mandible / jaw dislocation / TMJ subluxation is an infrequent A&E presentation.
The condition is discomforting to the patient, although most are not in severe pain. In the majority of cases, the mandible (lower jaw) can be reduced by the A&E staff using simple techniques. Rarely, a mandibular dislocation may require open reduction under general anæsthesia.
Once the condyle (see below diagram) comes out of its fossa, it comes to lie in front of the articular eminence and is mechanically blocked from spontaneously moving back into its correct position (in the fossa).
Spasm of the masseter and pterygoid muscles (chewing muscles) results in trismus (limited mouth opening) and further traps the condyle in its dislocated position. The resulting dislocation may be one sided or both. In either case, the patient will be unable to completely close the mouth and will often have difficulty speaking.
The dislocation is surprisingly not very painful unless an associated mandibular fracture is present.


Predisposing Factors for Jaw Dislocation:
- Most dislocations occur spontaneously on opening the mouth widely for yawn, dental work, during an epileptic seizure
- Trauma may also produce dislocation
- Trauma involving a downward force on partially opened jaw
- Those with previous dislocations are at much greater risk for repeat dislocation
- Shallow mandibular fossa may predispose to dislocation
- Connective tissue diseases like Marfan’s or Ehlers-Danlos may have increased risk
- May eventually result in osteoarthritis in TM joint
Clinical Findings:
- Dislocations of the lower jaw (mandible) tend to be uncomfortable but not severely painful for the patient
- The presence of a jaw fracture increases the pain
- Patients are unable to close mouth completely
- Difficulty speaking and, possibly, swallowing
- Dislocations may be one-sided or both (unilateral or bilateral)
- The lower jaw comes forward (pro-gnathic) appearance to jaw when both are dislocated
Imaging Findings:
- Conventional X-ray is usually diagnostic
- Mandibular condyle lies forward (anterior) to the articulate eminence on one or both sides
Reduction:
Once radiographs have been obtained that confirm a dislocation and exclude a mandibular fracture, reduction attempts may proceed. Patients with mandibular fractures should be referred to the OMFS Department. Uncomplicated dislocations can be managed in the A&E ± LA ± conscious sedation.
If the dislocation has just happened, no sedation or LA is needed. The longer the patient has been dislocated, the more likely either LA ± sedation or in more severe cases, GA.
Relocation:
An initial attempt can be made for the patient to self-relocate by eliciting the gag-reflex. Stimulation of the soft palate can induce the patient to gag. This can spontaneously re-locate the subluxed mandible.
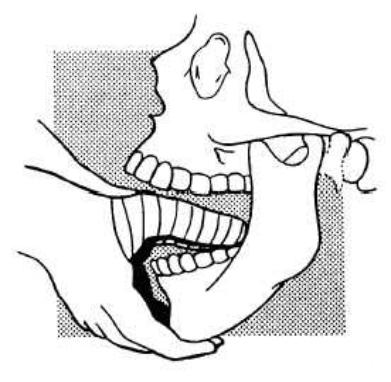
Gauze pads should be wrapped around both thumbs to prevent human bite injuries as the mandible is reduced. The thumbs are placed on the lower molars (or over the retro-molar pads) and the inferior surface of the mandible is grasped with the fingers on each side. Downward pressure is exerted on the lower molars to free the condyle from its entrapped position in front of the articular eminence.
Following this, the mandible is eased backwards to return it to its anatomic position. Successful reduction is usually evident as the teeth will close rapidly due to masseter spasm and a palpable (and sometimes audible) clunk occurs on reduction. The clinician must beware of having their thumbs being trapped in an inadvertent human bite as the mandible relocates.

Confirmation of relocation:
Repeat radiographs are indicated to confirm reduction and exclude the possibility of fracture during reduction.
The patient should be observed for airway patency and if sedation has been used, vital signs monitored until the effects of the sedatives have worn off.
The patient should be cautioned to avoid wide opening of the mouth to prevent recurrent dislocation. A Barton’s bandage is applied to prevent wide mouth opening and recurrent dislocation.
Follow-Up:
Further Inpatient Care:
In the rare cases of mandible dislocation that cannot be reduced by the method described above, attempted closed reduction under GA or open reduction may be required. Similarly, chronic dislocations or fractures / dislocations of the mandible are best reduced by OMFS or ENT specialists.
Further Outpatient Care:
Successfully relocated mandibular dislocations do not require any specific ongoing treatment, although the patient should be cautioned against wide opening of the mouth, which could easily cause a recurrence.
All patients with reduced mandibular dislocations should be followed-up by an appropriate specialist because of the possibility of jaw instability, ligamentous damage and chronic TMJ pain.
Complications:
Serious complications from mandibular dislocation are rare. There are several complications that are associated with the dislocation and reduction.
Dislocation complications:
Fracture of the mandibular condyle can occur during dislocation. Open fractures are at risk for infection and osteomyelitis. Interposition of soft tissues may make the dislocation irreducible.
Injury to the external carotid artery and facial nerve have been reported.
Complications of Reduction:
The clinician accomplishing the reduction may sustain a human bite as the jaw closes rapidly on reduction.
The mandibular condyle may fracture as it passes under the articular eminence.
Prognosis:
Because the dislocation occurs in anatomically predisposed individuals and disrupts the joint capsule and ligaments that stabilise the TMJ, recurrent dislocation is very common.
Recurrent dislocation often results in osteo-arthritis of the TMJ with chronic pain and inflammation.
There are many surgical interventions to correct chronic dislocation and painful TMJ syndrome that are described in the ENT literature. Because so many of the patients with mandible dislocation experience recurrent dislocation, it is advisable to refer all of these patients to an appropriate specialist for follow-up.
Patient Education:
Patients should be instructed to avoid opening their mouths widely to prevent recurrent dislocation
Useful Articles & Websites
Ind J Anaesth 2004. Temporomandibular Joint (TMJ) Dislocation During LMA Insertion
Pakistan Oral & Dent J 2008. Treatment of TMJ Recurrent Dislocation through Eminectomy – A Study
JOMS 2009. Autologous Blood Injection for the Treatment of Chronic Recurrent TMJ Dislocation
BJOMS 2012. Technical Note. Intra-Oral High Condylotomy for a Case of Chronic Mandibular Dislocation